By Marc Sorenson, EdD Sunlight Institute…
I recently happened across new research that should be of interest to those who love the Sun. It gave a historical perspective of TB that showed how the city of Bern, Switzerland wiped out most of their tuberculosis (TB) problems by using lifestyle changes, including a greater accessibility to sun.[1]
The authors studied the TB incidence in Bern during the period from 1856-1950. There were three areas of the city that were assessed for their historical TB problems. One was known as the Black Quarter, and in 1911 -1915 there were 550 cases per 100,000; another area was known as the City Center and had 327 cases per 100,000; a third area was known as the Outskirts, and had 209 cases per 100,000.
There were three living conditions that correlated closely to TB:
- Number of persons per room. A higher number predicted a greater risk of TB.
- A higher number of rooms without sunlight predicted a greater risk of TB.
- The number of windows per apartment predicted a diminished risk of TB
As the country worked to address these problems by improving living conditions, reducing room crowding, building open-air schools and building sanatoria, TB risk dropped from 330 cases per 100,000 in 1856 to 33 per 100,000 in 1950—a 90% drop! Sanatoria, by the way, were secluded hospitals that healed through good food, fresh air and sunlight.
The researchers concluded their paper with this statement: “Improved living conditions and public health measures may have contributed to the massive decline of the TB epidemic in the city of Bern even before effective antibiotic treatment became finally available in the 1950s.”
This is an important paper. It shows that natural methods, including sun exposure, were highly effective in decimating TB. Sanatoria may be needed again, as the superbugs, including TB superbugs, are now highly resistant to antibiotics.[2]
When the people avoid the sun, they set themselves up for disease. Instead, embrace the sun, but don’t burn. It is one of the best methods of disease prevention known to man, and it doesn’t produce any superbugs; in fact it kills them!
[1] Zürcher K, Ballif M, Zwahlen M, Rieder HL, Egger M, Fenner L. Tuberculosis Mortality and Living Conditions in Bern, Switzerland, 1856-1950. PLoS One. 2016 Feb 16;11(2):e0149195
[2] Moisse, K. Drug Resistant TB could bring back Sanatoria. ABC News October 2011.
By Marc Sorenson, EdD Sunlight Institute…
Research from Singapore, a very sunny country, demonstrated that 57% of older adults with hip fractures were vitamin D deficient.[1] The researchers note that in Western countries with seasonal winters, D deficiency is common due to the reduction in sunlight. But on measuring serum vitamin D in fracture patients in sunny Singapore, they found that 57.5% were suffering deficiency and 34.5% were suffering insufficiency. Only 8% of the patients had normal vitamin D levels.
One might ask why people residing in a sunny, predominantly tropical climate would have such a high degree of vitamin D deficiency and consequently high fracture risk. Further study found the answer: Most of the people who suffered fractures had been housebound and had little sun exposure. The authors of the paper made the following statement: “Another factor was Malay ethnicity (dark skin, which inhibits vitamin D production), and clothing habits that prevented sun exposure.”
The authors of the paper concluded with this statement: “Vitamin D deficiency and insufficiency are common in patients with hip fracture in Singapore. Vitamin D deficiency was associated with being housebound and those of Malay ethnicity. Clothing habits resulting in reduced sunlight exposure may increase the risk of vitamin D deficiency.”
The same pattern of high D deficiency also exists among youth in some sunny countries; in Qatar deficiency is common. [2] Sixty-eight percent of the children there are deficient and the girls are especially likely to be deficient. Low duration of time spent outdoors is a major predictor of deficiency, and the children who are deficient suffer a greater incidence of rickets, fractures, and gastroenteritis.
And finally, I would like to remind the readers of research from Spain that I have cited on various occasions. Women who spend their time indoors are about 11 times more likely to have a fracture as those who regularly seek the sun.[3]
A major message is this: If the sunlight is all around you and you don’t expose yourself to it, it will do you no good. You may a well live in the Arctic Circle.
Carefully embrace the sun and save your bones.
[1] Ramason R, Selvaganapathi N, Ismail NH, Wong WC, Rajamoney GN, Chong MS. Prevalence of vitamin D deficiency in patients with hip fracture seen in an orthogeriatric service in sunny Singapore. Geriatr Orthop Surg Rehabil. 2014 Jun;5(2):82-6
[2] Bener A, Al-Ali M, Hoffmann GF. High prevalence of vitamin D deficiency in young children in a highly sunny humid country: a global health problem. Minerva Pediatr. 2009 Feb;61(1):15-22.
[3] Larrosa M, Casado E, Gómez A, Moreno M, Berlanga E, Ramón J, Gratacós J. Vitamin D deficiency and related factors in patients with osteoporotic hip fracture. Med Clin (BARC) 2008;130:6-9.
By Marc Sorenson, EdD. Sunlight Institute…
In end stage kidney disease, heart disease and other vascular diseases are often the most dreadful accompanying disorders, also known as a comorbidities. Any healthful procedure that can mitigate the distress of these diseases can be a godsend to the patient suffering from kidney deterioration. UV therapy, similar to sun exposure, has now been shown to alleviate some of the difficulties of cardiovascular diseases and thereby increase the quality of life.[1]
The research was conducted on fourteen kidney-dialysis patients. They were irradiated with whole-body UV for six months. Before and after that time, they were measured for several physiological functions to determine if there had been worthwhile changes in indicators of cardiovascular diseases. These were the results:
- Hematocrit increased, indicating a larger volume of red blood cells, which are important for carrying oxygen to the heart, vessels and all other parts of the body.
- The patients required less erythropoietin, a hormone that stimulates production of red blood cells and hemoglobin in case of low-tissue oxygen. This would indicate that oxygen need was reduced after the UV treatment, putting less stress on the cardiovascular system.
- In addition to, or perhaps because of, these positive changes, maximal oxygen uptake increased, indicating greater work capacity and physical fitness.
- Workload capacity increased and lactic acid production decreased, also indicative of enhanced physical fitness.
- Pulse rate decreased, indicative of an ability of the heart to deliver more oxygen per beat through the cardiovascular system. This is also a fitness measurement.
- Both systolic and diastolic blood pressures decreased, showing a healthier vascular system.
The researchers made the following conclusion: “Cardiovascular disease is the most important comorbidity [to kidney disease]. Exposure to simulated sunlight that contains both UVB and UVA reduce cardiovascular risk factors and improve quality of life.”
Protect your kidneys or protect your heart either by safe exposure to the “simulated sunlight” of sunlamps or tanning devices, or by regularly exposing yourself (again, safely) to mankind’s best friend the Sun.
[1] Krause R, Stange R, Kaase H, Holick MF. UV Irradiation and Pleiotropic Effects of Vitamin D in Chronic Kidney Disease – Benefits on Cardiovascular Comorbidities and Quality of Life. Anticancer Res. 2016 Mar;36(3):1403-8.
By Marc Sorenson, EdD. Sunlight Institute…
Part 2. The assault on the Sun: Dishonesty, duplicity and dollars
Attacking the sun makes $millions, and there is a war going on. The combatants are The Sun vs. The Powers of Darkness (those who have a financial interest in disparaging the sun).
As discussed earlier, the American Academy of Dermatology (AAD) published a report showing that most melanoma diagnoses may be incorrect, showing that only about 6% of melanoma diagnoses resulted in actually being melanoma.[1] They also published information on a vitamin D/melanoma study demonstrating that the lowest vitamin D levels were associated with a 500% increase in the risk of melanoma.[2] Of course, they would never admit that sun-derived vitamin D would help. We have already presented incontrovertible evidence that regular or habitual sun exposure is associated with a profoundly reduced risk of melanoma. Yet, the AAD and other organizations in the Power of Darkness cabal continue to repeat the tiresome advice to completely avoid any direct sun exposure. Meanwhile, people die while the AAD has fun in the sun–the height of hypocrisy. Here are two pages, touting their meetings, from Dermatology World, the organ of the Association, taken from Dr. Bernard Ackerman’s marvelous and massive monograph against his own profession, entitled The Sun and the “Epidemic” of Melanoma: Myth on Myth.[3]
I find it strange that San Diego and San Antonio, with their abundant sun, would be chosen for their “scientific” meetings. Obviously they do not believe their own messages, but disseminate those messages to help line their pockets while they enjoy the “sun and surf.” Can you trust them?
Dr. Ackerman, a celebrated dermatologist, also made the following statement in his monograph: “…the sun, now incriminated as the major culprit responsible for an “epidemic” of melanoma, will be rehabilitated from its status current of pariah, our worst enemy, to its place rightful, all things considered, namely, humankinds best friend.”
Dr. Ackerman also exposed the influence that money plays among the purveyors of the anti-sun movement and the makers of sunscreens. He states that …”the American Academy of Dermatology, the Skin Cancer Foundation and the American Cancer Society sold their seals of recommendation to manufacturers of sunscreen, the price being substantial in terms of dollars but incalculable in regard to tarnish of honor.”
He adds that the for an application fee of $10,000 (now reduced to $5,000) and an annual fee of $10,000, a sunscreen manufacturer can boast approval of its product in the form of the “Seal of Recognition” of the American Academy of Dermatology that decorates the front of tubes. The Skin Cancer Foundation has done the same for many years, and the “sunscreen companies pay it many thousands of dollars annually in the hope of gaining many millions of dollars in return.
He tells us that the “vaunted American Cancer Society (ACS) displays its logo on the front of tubes of Neutrogena for $300,000 annually.”
One great examples of this duplicity is displayed in the ad below, which was run in women’s magazines, ostensibly paid for by the American Cancer Society (ACS). The ACS logo appears in the lower right corner, making it appear that the ad was purchased by the ACS. It serves as a sales pitch for sunscreens by saying “Use sunscreen, cover up and watch for skin changes.” Additionally, the ad shows a young woman stating that “My sister accidentally killed herself. She died of skin cancer.” 
Now let’s examine the truth about this ad, as uncovered by the New York Times.
1. This ad was not sponsored nor paid for by the ACS. It was paid for by Neutrogena—a convenient way to sell sunscreens without letting the public even know that the ad is anything more than a public-service announcement. And shame on the ACS for selling their souls for filthy lucre.
2. The picture being held by the young lady is not a picture of her sister, and the young woman herself is a model hired to pose for the ad. More deception and more dollars changing hands.
This chicanery is done for one purpose only: Money from sales of sunscreens. More on that subject in a future post. Until then enjoy the sun safely, and do not burn.
[1] Argenziano G1, Cerroni L, Zalaudek I, Staibano S, Hofmann-Wellenhof R, et al. Accuracy in melanoma detection: a 10-year multicenter survey. J Am Acad Dermatol. 2012 Jul;67(1):54-9.
[2] No authors. Vitamin D May Protect Against Some Melanomas. Annual meeting of the American Academy of Dermatology, February 15, 2011, reported in Skin and Allergy News.
[3] Ackerman, B. The Sun and the “Epidemic” of Melanoma: Myth on Myth. 2008.
By Marc Sorenson, EdD. Sunlight Institute…
Most of the following Material is excerpted from my upcoming book, Embrace the Sun, which will be available sometime this summer.
The assault on the sun, which has increased in intensity for several decades, is one of the most heinous crimes yet perpetrated on humanity. At the root of this evil is the love of money, as is the case in most instances where large numbers of people are defrauded by business entities in collusion with government and “education.” When these forces combine to use half-truths, outright falsehoods and chicanery that destroy health and shorten lives, are they not engaging in high crimes and misdemeanors? What do we call the crime of taking away another’s life? I am opposed to evil in all its forms, including the theft of sun—a theft that diminishes the mental, spiritual and physical advantages sun brings to mankind. The lies perpetuated by supposedly professional organizations make me ill.
I do not oppose making money in an honest manner. The desire for money, and therefore for a better life, is one of the engines that drives entrepreneurship and leads to the marvelous technologies that we enjoy. But money that derives from lying to the people indicates that evil is at play. When a business finds that one of its products (or messages) is causing harm that could literally lead to disease and death, its first act should be to inform its customers and distributors, and then it should remove the product or message from the market. Regrettably, cover-ups and arguments against such findings are often the norm. The first thought is not “We must warn the people that our product or message is harmful,” but rather, “We must do damage control so that our cash flow is not interrupted.” Indeed, if the product is being unjustly maligned, a vigorous campaign against such malignity should be undertaken; but if the complaint against the product is just, then honesty in correcting the problem or eliminating the product should be the first step.
As regards the sun, it has been assailed from many sides as being the plague of mankind—a devastating scourge that is resulting in a plethora of skin diseases—especially melanoma, that threaten to destroy life on Earth. And despite voluminous research to the contrary, the mantra of those who market sunscreens and (most) of those who treat melanoma remains, “Cover up, avoid sun exposure and never forget to use your sunscreens.” Accordingly, the blood is on their hands; they have a billion-dollar business to support, and the facts be damned.
The anti-sun organizations such as the American Academy of Dermatology (AAD) and the Skin Cancer Foundation (SCF) have been spreading a false message for decades. Their pundits have claimed that the sun is public health enemy number 1 and should be avoided at all costs. They have raised the alarm that melanoma would become the scourge of mankind unless steps were taken to remove the presence of sun exposure from human existence.
Perhaps you will believe that the above statement is outlandish hyperbole. But consider two statements by Wilma Bergfeld, a former president of the AAD, in 1996:
- Melanoma will be the leading cause of cancer death among Americans by 2012.
- Mankind will need to move underground to survive the hazards of sun exposure, namely melanoma.
If you would like to hear the words that emanated from her mouth, view the short video below.
How could anyone believe the propaganda promulgated by Dr. Bergfeld, which is still being pushed by the AAD? Nevertheless, the drumbeat to avoid the sun is having its impact, as death, disease and destruction follows in the wake of its “education” programs.
Let’s consider some truths regarding sun exposure and melanoma.
The Melanoma International Foundation (MIF) states that ultraviolet radiation (UVR) from sun causes melanoma and should be avoided as a detriment to human health.[1] That message is primarily disseminated by (some) dermatologists and their governing bodies (previously discussed), which conveniently ignore the hundreds of scientific investigations associating sun exposure to profoundly better health. The sun performs its miracles by reducing risk for such maladies as breast and prostate cancer, heart disease, osteoporosis and scores of others. The MIF message does not differentiate between strong, intermittent exposure, which can lead to sunburn, and regular, non-burning exposure, such as that received by those who routinely work and recreate outdoors. As you will shortly read, the latter are protected against melanoma.
Concomitantly, a message that opposes the MIF statement is rapidly emerging: sun avoidance, by reducing the body’s production of vitamin D and other beneficial photoproducts, is responsible for a dramatic increase in both degenerative and communicable diseases.[2] In addition, a third view is drawing adherents: that the increase in melanoma incidence is an illusion and an artifact produced by incorrect assessment: the misdiagnosis of benign skin lesions as melanoma.[3]
Nevertheless, melanoma is nothing to trifle with, and any unusual skin lesion should be immediately assessed by a dermatologist. However, since many lesions are benign, yet may nonetheless be misdiagnosed as melanoma, it is a good idea to seek multiple opinions before an excision is performed. Proceeding through a deep and invasive surgery for a harmless lesion is something no one should experience, and the most harmful part of the surgery may be the needless fear that one could have died from a deadly cancer—a cancer that really never existed.
Melanoma accounts for about 9,940 cancer deaths per year in the U.S., making up only a small portion of the total number of cancer deaths per year in the US, estimated to be 589,430.[4] Interestingly, melanoma is most common among men over 50,[5] which makes one wonder why tanning beds are being targeted for extinction by the dermatological societies. Men over 50 hardly fit the demographic that use tanning beds! That demographic is young women. Already we begin to see that there is deception within the organizations that promote sun avoidance; the mantra continues to be that we are killing our young women with tanning-bed use and sun exposure. Does no one care for the 50-year-old men who are dying from melanoma and do not use tanning beds? Does anyone even mention that there are more than twice as many men as women who die from melanoma?[6]
It has been ingrained into the consciousness of educated people throughout the world that the ultraviolet portion of sun radiation (UVR) is the cause of melanoma. The world population, however, as it “progresses,” spends increasingly less time exposed to direct sun. This is due to (1) an increase in indoor activities and decrease in outdoor activities, and (2) the increased use of sunscreens to prevent UVR exposure when outdoors. Nevertheless, the rate of melanoma is believed to be increasing at an alarming pace, as evinced by the aforementioned statement by the MIF, who also stated in 2007 that “melanoma is epidemic: rising faster than any other cancer and projected to affect one person in 50 by 2010, currently it affects 1 in 75. In 1935, only one in 1,500 was struck by the disease.”[7] That is correct; the American Cancer Society in 2014 reported that one in 50 now contracts the disease.[8] The MIF, then, if one assesses the statistics reported by medical organizations, was accurate regarding the increase in melanoma. However, they were wrong, perhaps “dead wrong” in stating that the sun is at fault.
Let’s take another look at the mathematics. According to the MIF, people had about 30 times the risk of contracting melanoma in 2010-2014 as in 1935, or stated in another way, a 3,000% risk increase. One might surmise that sun exposure must have increased spectacularly, during the time frame discussed, to have caused the exponential increase in melanoma, assuming that the statement by the MIF—that melanoma is caused by sun exposure—is correct. But is that statement correct?
Let’s ask six pertinent questions.
Question 1. Has sun exposure increased as melanoma has increased?
If melanoma has indeed increased exponentially since 1935, and if that increase is due to sun exposure, then sun exposure must also have shown a parallel or at least significant increase during that time. To determine the veracity of that idea, I analyzed data from the Office of Occupational Statistics and Employment Projections, Bureau of Labor Statistics (BLS), to determine if there was an increase or a decrease in human sun exposure during the years from 1910 to 2,000.[9] I closely considered changes since 1935, the year the MIF used as a baseline for measuring increases in melanoma incidence.
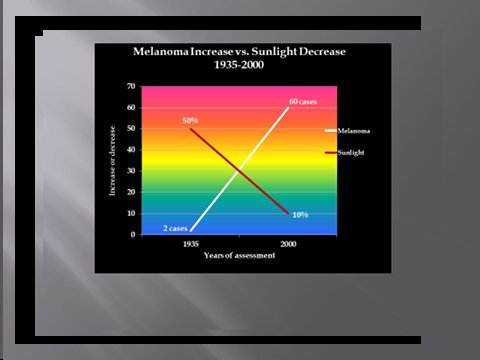
The data from the BLS showed that indoor occupations such as “professional, managerial, clerical, sales, and service workers (except private household service workers) grew from one-quarter to three-quarters of total employment between 1910 and 2000.” The BLS also stated that during the same period, the outdoor occupation of farming declined from 33% to 1.2% of total employment, a 96% reduction. The data also show that approximately 66% of the decline in the occupation of farmers and 50% of the decline in the occupation of farm laborers occurred after 1935. Further information, this time from the Environmental Protection Agency (EPA) determined that as of 1986, about 5 percent of adult men worked mostly outside, and that about 10 percent worked outside part of the time. The proportion of women who worked outside was thought to be even lower.[10] These data demonstrate a dramatic shift from outdoor, sun-exposed activity to indoor, non-sun-exposed activity during the mid-to-late 20th Century. This change, nonetheless, has been accompanied by a 30-times increase in melanoma risk since 1935, the MIF-baseline year. Accordingly, if sun exposure is really responsible for the pandemic of melanoma, it has achieved that dubious distinction during a time of profound decrease in sun exposure! To me, this is wholly counterintuitive. The data just presented really suggest that sun exposure is not responsible for the increase in melanoma, and we submit instead, that the profound decrease in sun exposure may be a factor in the purported exponential melanoma increase. That concept is illustrated graphically below.
Although it has been theorized that decreasing thickness of the ozone layer may be responsible for the increasing incidence of melanoma, research by Moan and Dahlback in Norway reported that yearly melanoma incidence increased 350% in men and 440% in women between 1957 and 1984—a period when there was absolutely no thinning of the ozone layer.[11]
The answer to question 1 is no; sun exposure has not increased as melanoma has increased. Exactly the opposite has occurred.
Question 2. Do outdoor workers have a higher incidence of melanoma than indoor workers?
If melanoma is increasing due to increased sun exposure, it is clear that outdoor workers, being exposed to far higher quantities of sun, would also have a far higher incidence of melanoma. Nevertheless, Dianne Godar and colleagues[12] presented evidence that outdoor workers, while receiving 3-9 times the sun exposure as indoor workers have had no increase in melanoma since before 1940, whereas melanoma incidence in indoor workers has increased steadily and exponentially.[13] [14]
Godar and colleagues also published irrefutable evidence of the protective influence of sun against melanoma in a landmark study in 2015,[15] entitled Dramatic Increases in Melanoma Correlate to Low Annual Sun exposure in Europe.
Published in the scientific journal Dermato-Endocrinology, the paper makes some very interesting comments, all based on excellent research:
- Melanoma has steadily increased in fair-skinned indoor working people around the world. Increasing melanoma incidence significantly correlates with decreasing personal annual UV doses [emphasis ours]. (UV or ultraviolet radiation is the spectrum of sun that stimulates the skin to produce vitamin D3.)
- People are more susceptible to melanoma when they have larger numbers of moles, light skin and hair, and poor tanning ability.
- There is a paradox between indoor and outdoor workers’ melanoma incidences and their annual UV (ultraviolet light) exposure. Outdoor workers receive 3-9 times the annual UV doses that indoor worker receive, but have only 50% of the risk for contracting melanoma.
- Although most scientists believe that intermittent UV exposures—resulting in sunburns—initiate melanoma, the creation and use of sunscreens DID NOT [emphasis ours] reduce the incidence of the disease. One of the reasons may be that sunscreens dramatically reduce vitamin D synthesis in the skin.
- Sunburns are probably not [emphasis mine] involved in the initiation or growth of melanoma, since a study on opossums showed that intense sun doses of UVB produced significantly fewer melanomas than sub-erythemal (non reddening) doses. Also, outdoor workers do get numerous sunburns but still have dramatically lower risk of contracting melanoma. [I do not advocate sunburning; although it may not cause melanoma, it will certainly do some damage to skin.]
- Many melanomas occur on areas of the body where the sun never shines.
The authors go on to theorize that a lower level of vitamin D, among those who receive inadequate sun, could be a major reason for the exponential increase of melanoma in European countries where the UV (sun) exposure is minimal. Another reason they suggest is infection with human papilloma virus (HPV).
Whatever the theories propose, regarding the cause of high melanoma incidence accompanying low sun or UV exposure, the equation remains the same: FOR THE VAST MAJORITY OF THE POPULATION, THE GREATER THE REGULAR EXPOSURE TO SUN, THE LESS THE RISK OF MELANOMA. Nevertheless, such information sells neither sunscreens nor melanoma surgeries, so don’t stand on one leg until the public believes the truth. However, you can learn the facts and become a soldier in the “sun army” by promoting the evidence.
Other research corroborates the idea that outdoor workers experience less melanoma than indoor workers.[16] Vagero, et al.[17] showed that melanoma was more common among indoor office workers and other indoor workers than among outdoor workers, and Kennedy, et al.[18] showed that a lifetime of sun exposure correlated to a reduced risk of melanoma. Garland, et al.[19] showed that those who worked indoors had a 50% greater risk of melanoma than those who worked both indoors and outdoors, and Kaskel, et al.[20] demonstrated that children who engage in outdoor activities are less likely to develop melanoma than those who do not. Many other papers in the scientific literature show that both incidence and death rate from melanoma are reduced with increasing exposure to sun.[21] [22] [23] [24] [25] [26] [27] [28] [29] [30] [31] [32]
None of these findings is surprising when one considers that whereas common, non-melanoma skin cancers are easily produced in experiments using ultraviolet radiation (UVR) from sunlamps, the same is not true for melanoma, which is difficult to produce with UVR.[33]
Finally, from 2016, research reported in the journal Anticancer Research demonstrated that UVR exposure was inversely associated with melanoma.[34] The researchers had set out to study whether the annual UVR level, estimated on a county level, was associated with incidence rates of oral, pharyngeal, and cervical cancers and melanoma. They found that all of these cancers were inversely associated with sun exposure. Interestingly, the authors, in their introduction to the research, said that UVR exposure is a well-demonstrated risk factor for melanoma. Then, at the end of their paper, they made this statement: “Our findings are in agreement with several other published studies reporting no positive correlation between UVR exposure and the incidence rates of oral, pharyngeal, and cervical cancer and melanoma.” Those two statements are contradictory, but their conclusion was correct: Those cancers are inversely correlated to UVR. Do you believe that the anti-sun organizations will admit their errors and embrace the sun? Don’t bet your bank account on it!
This data indicate again that sun exposure is not responsible for the increase in melanoma, and that the decrease in sun exposure may be a factor in the reported dramatic melanoma increase.
The answer to question 2 is no; outdoor workers do not have a higher incidence of melanoma than indoor workers.
Question 3. Do many melanomas occur on areas of the body that receive little sun exposure?
If sun exposure is the reason for the increase in melanoma, then it would be reasonable to expect that areas of the body that receive the most exposure, would also be the areas of greatest occurrence of the disease. This is not the case. The research by Garland and colleagues al.,[35] when assessing the incidence of melanoma occurring at various sites, found higher rates on the trunk (seldom exposed to sun) than on the head and arms (commonly exposed to sun). Others have shown that melanoma in women occur primarily on the upper legs, and in men more frequently on the back—areas of little sun exposure.[36] In blacks, melanoma is more common on the soles of the feet and on the lower legs.[37] Based on this data, it would be difficult to make the case that sun exposure is responsible for the increase in melanoma.
It should be mentioned that it is believed that intermittent bursts of intense sun (that causes sunburn) increases the risk of melanoma, whereas regular exposure reduces the risk[38] and that even on chronically sun-damaged skin, the mutations that lead to melanoma are rare.[39] Even the idea that sunburn causes melanoma is inconsistent with the fact that most melanomas do not occur at burn sites.[40] [41] The paper by Godar[42]put forth the hypothesis that lack of sun reduces the quantity of vitamin D in the skin, and then cited research showing that the potent hormone form of vitamin D, calcitriol, reduced the incidence, size and number of skin tumors and also reduced invasiveness and metastasis of melanoma in mice. Since regular sun exposure correlates to higher vitamin D production and higher levels in the blood, this evidence is plausible and would explain the reasons for reduced melanoma rates among those who are regularly exposed to sun.
Since many melanomas occur on areas of the body that receive little sun exposure, the indication is that sun exposure is not the cause of melanoma.
The answer to question 3 is yes, many melanomas occur on areas of the body that receive little sun exposure.
Question 4. Is there a co-morbidity of melanoma with common skin cancers, some of which are known to be associated to high sun exposure?
There is general agreement that sun exposure is one of the causal factors for squamous cell and basal cell carcinoma, also known as non-melanoma skin cancer (NMSC). However, these cancers do not demonstrate co-morbidity with melanoma.[43] [44] [45] Dr. Grant, after analyzing data from the Atlas of Cancer Mortality in the United States, noted that between 1950-1969 and 1970-1994, death rates from NMSC decreased by 31% for white males and by 47% for white females. However, during those same periods, melanoma death rates increased by 89% in white males and 42% for white females.[46]If one accepts the rate of NMSC as a measure of the cumulative exposure to sun, it is reasonable to conclude that sun exposure correlates to a reduced risk of melanoma, and that the lack of exposure increases the risk of melanoma.
This is another indication that sun exposure is not responsible for the increase in melanoma.
The answer to question 4 is no; there a no co-morbidity of melanoma with common skin cancers, some of which are known to be associated to high sun exposure.
Question 5. Has an increase in sunscreen use resulted in a decrease in melanoma?
Sunscreens block sun, and they are intended to decrease sun damage to the skin—damage that is said to increase the risk of melanoma. Sunscreen use has increased considerably in the past few decades. Therefore, if sun exposure is the cause of melanoma—as stated by the IMF—there should be a simultaneous decrease in melanoma as sunscreen use has increased. According to Kline & Company, a research group, sales of sunscreens in 1972 were $33 million; in 2008, sales were $650 million.[47] In addition, according to the Fredonia Market Research Group Company, the sales of sunscreens used in cosmetics in 2007 was $130 million.[48] Therefore, the total sales of sunscreens as of 2007 were $780 million. Considering that a dollar’s value is only about 20% of what it was in 1972, the adjusted 2008 sunscreen expenditures are approximately $156 million, or about 4.7 times the 1972 figure. In other words, sunscreen use has increased by about 4.7 times. Population also grew from 210 million in 1972 to 305 million in 2008–a 50% increase. Adjusting for population growth, it can be concluded that per capita sunscreen use has at least tripled in the time frame being considered.
As previously discussed, melanoma, according to the MIF, has increased steadily and exponentially since 1935. Therefore, the data on increasing sunscreen use does not indicate that sun exposure increases the risk of melanoma. Rather, it indicates that sunscreen use may, by reducing vitamin D production, contribute to the reported increase in melanoma. It has been shown that an SPF 15 sunscreen will decrease sun-stimulated vitamin D production by 99.5%, [49]and it has been suggested that by blocking only UVB light (which stimulates the production of vitamin D in skin) while leaving UVA unblocked, sunscreens ironically may lead to UVA damage of DNA, leading to melanoma.[50] [51] Increasing melanoma rates, coupled with increasing use of sunscreen, lends credence to that hypothesis. Regular sun exposure, therefore, does not increase risk of melanoma.
The answer to question 5 is no; increase in sunscreen use has not resulted in a decrease in melanoma.
Now let’s ask one more very important question:
Question 6. Is it possible that the reported pandemic of melanoma is not a pandemic at all, but that the “increase” in melanoma” is due to excessive diagnosis of benign lesions?
Writing in the British Medical Journal in 2008, Dr. Sam Shuster, a dermatologist, argued that the purported increase in melanoma is not really an increase, but an artifact due to non-melanoma lesions being misdiagnosed as melanoma.[52] In 2009, another study by dermatologists— Shuster and his colleagues—this time published by the British Journal of Dermatology, came to a similar conclusion and called the “increase” in melanoma a “midsummer night’s dream.”[53] They concluded, after tracking the reported increase in melanoma in the Eastern region of the UK between 1991 and 2004, that benign lesions were being classified in increasing numbers as stage-one melanoma. No other stages of the disease increased, and the increase in mortality due to melanoma was either miniscule or non-existent. This was true even though all grades of tumors were diagnosed at first presentation. They also noted that “the distribution of the lesions reported did not correspond to the sites of lesions caused by solar exposure,” a finding similar to that discussed in heading #3 above. These dermatologists concluded that “the large increase in reported incidence is likely to be due to diagnostic drift which classifies benign lesions as stage 1 melanoma.” They further stated that “These findings inevitably challenge the validity of epidemiology studies linking increasing melanoma incidence with UV radiation and suggest the need for a search for other ways in which the disease may be caused.”
Another celebrated dermatologist, Dr. A Bernard Ackerman, has written a monograph entitled Sun and the “Epidemic” of Melanoma: Myth on Myth.[54] In it he reviews extensive research and concludes that melanoma has nothing to do with sun exposure; and like the authors of the aforementioned BMJ article, he indicates that excessive diagnosis of benign lesions is responsible for the purported epidemic of melanoma.
Stunningly, the American Academy of Dermatology (AAD) published a report showing that most melanoma diagnoses may be incorrect.[55]Approximately 44 different authors contributed to that report. They made an accuracy-in-detection analysis based on the number of melanomas that needed to be excised during a period of ten years, compared to the actual number that were excised. Many clinics in different countries were involved in assessing the numbers.
A total of 300,215 cases were found where excision took place. Of those cases, there were 17,172 melanomas that really required excision, and 283,043 that were excised and turned out to be benign lesions. Therefore, there were about 16.5 non-melanoma lesions removed for each lesion that was cancerous, and only about 6% were legitimate cancers. From this information, it is obvious that many melanoma surgeries are bogus and may inflate the incidence of melanoma. The aforementioned Drs. Shuster and Ackerman were correct. Dermatology is a huge business, and considering the spectacular per capita increase in the number of dermatologists, it is no wonder that they want to keep this little gravy train rolling down the track. See the graph below, which illustrates that the increase in the numbers of dermatologists paralleld the increase in the number of melanomas in young women.

It is obvious that the business of removing benign lesions is lucrative for the doctors. As the authors stated in their introduction to their research, “Early excision is the only strategy to reduce melanoma mortality, but unnecessary excision of benign lesions increases morbidity and healthcare costs.” It is hard to believe that the AAD published the report, but I am thankful it was done.
The answer to question 6 is yes. It is possible that the reported pandemic of melanoma is not a pandemic at all, but that the “increase” in melanoma” is due to excessive diagnosis of benign lesions.
The bottom line: From the research thus far presented, it could be concluded that either melanoma is increasing dramatically and is directly correlated to decreasing sun exposure, or that melanoma is not increasing at all, and the “epidemic” of melanoma does not exist. In either case, the statement by the MIF—that sun causes melanoma—has no validity. Stop blaming the sun!
You should have learned the following points from this part of the presentation:
- Sun exposure has decreased profoundly as melanoma has increased remarkably.
- Outdoor workers have a significantly lower incidence of melanoma than indoor workers.
- Many melanomas occur on areas of the body that receive little or no sun exposure.
- There a no co-morbidity of melanoma with common skin cancers, some of which are known to be associated to high sun exposure.
- An increase in sunscreen has been associated with an increase in melanoma incidence.
- It is possible that the “epidemic” of melanoma is not an epidemic at all, but that the “increase” in melanoma is due to excessive diagnosis of benign non-melanoma lesions.
- The idea that regular sun exposure leads to melanoma is counterintuitive.
- These facts should be presented to everyone who defames the sun as a carcinogen (cancer causer) for melanoma.
Stay tuned for more posts on this subject.
[1]Melanoma International Foundation, 2007 Facts about melanoma. Sources: National Cancer Institute 2007 SEER Database, American Cancer Society’s 2007 Facts and Figures, the Skin Cancer Foundation, the American Academy of Dermatology.
[2]Grant, W. In defense of the sun: An estimate of changes in mortality rates in the United States if mean serum 25-hydroxyvitamin D levels were raised to 45 ng/mL by solar ultraviolet-B irradiance. Dermato-endocrinology 2009;4:207-214.
[3]N.J. Levell, C.C. Beattie, S. Shuster and D.C. Greenberg. Melanoma epidemic: a midsummer night’s dream? British J Dermatol 2009;161:630–34
[4]Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015.CA Cancer J Clin. 2015 Jan-Feb;65(1):5-29.
[5] Melanoma Research Foundation. Melanoma Fact Sheet. Accessed 9-15-2014 at http://melanomainternational.org/melanoma-facts/#.VCHCG1_ANE0
[6] American Cancer Society. Cancer Facts & Figures 2015
[7] Melanoma Research Foundation. Melanoma Fact Sheet. Accessed 9-15-2014 at http://melanomainternational.org/melanoma-facts/#.VCHCG1_ANE0
[8] American Cancer Society. Melanoma Skin Cancer Overview 9/16/2014. http://www.cancer.org/cancer/skincancer-melanoma/overviewguide/melanoma-skin-cancer-overview-key-statistics
[9] Ian D. Wyatt and Daniel E. Hecker. Occupational changes in the 20th century. Monthly Labor Review, March 2006 pp 35-57: Office of Occupational Statistics and Employment Projections, Bureau of Labor Statistics
[10] U.S. Congress, Office of Technology Assessment, Catching Our Breath: Next Steps for Reducing Urban Ozone, OTA-O-412 (Washington, DC: U.S. Government Printing Office, July 1989).
[11] J. Moan and A. Dahlback. The relationship between skin cancers, solar radiation and ozone depletion. Br J Cancer 1992; 65: 916–21
[12] Godar D, Landry, R, Lucas, A. Increased UVA exposures and decreased cutaneous Vitamin D3 levels may be responsible for the increasing incidence of melanoma. Med Hypotheses 2009;72(4):434-43.
[13] Godar D. UV doses worldwide. Photochem Photobiol 2005;81:736–49.
[14] Thieden E, Philipsen PA, Sandby-Møller J, Wulf HC. UV radiation exposure related to age, sex, occupation, and sun behavior based on time-stamped personal dosimeter readings. Arch Dermatol 2004;140:197–203.
[15] Stephen J Merrill, Samira Ashrafi, Madhan Subramanian & Dianne E Godar. Exponentially increasing incidences of cutaneous malignant melanoma in Europe correlate with low personal annual UV doses and suggests 2 major risk Factors. Dermato-endocrinology 2015;7:1
[16] Lee J. Melanoma and exposure to sun. Epidemiol Rev 1982;4:110–36.
[17] Vågero D, Ringbäck G, Kiviranta H. Melanoma and other tumors of the skin among office, other indoor and outdoor workers in Sweden 1961–1979 Brit J Cancer 1986;53:507–12.
[18] Kennedy C, Bajdik CD, Willemze R, De Gruijl FR, Bouwes Bavinck JN; Leiden Skin Cancer Study. The influence of painful sunburns and lifetime sun exposure on the risk of actinic keratoses, seborrheic warts, melanocytic nevi, atypical nevi, and skin cancer. Invest Dermatol 2003;120:1087–93.
[19] Garland FC, White MR, Garland CF, Shaw E, Gorham ED. Occupational sun exposure and melanoma in the USA Navy. Arch Environ Health 1990; 45:261-67.
[20] Kaskel P, Sander S, Kron M, Kind P, Peter RU, Krähn G. Outdoor activities in childhood: a protective factor for cutaneous melanoma? Results of a case-control study in 271 matched pairs. Br J Dermatol 2001;145:602-09.
[21]Garsaud P, Boisseau-Garsaud AM, Ossondo M, Azaloux H, Escanmant P, Le Mab G. Epidemiology of cutaneous melanoma in the French West Indies (Martinique). Am J Epidemiol 1998;147:66-8.
[22]Le Marchand l, Saltzman S, Hankin JH, Wilkens LR, Franke SJM, Kolonel N. Sun exposure, diet and melanoma in Hawaii Caucasians. Am J Epidemiol 2006;164:232-45.
[23]Armstong K, Kricker A. The epidemiology of UV induced skin cancer. J Photochem Biol 2001;63:8-18
[24]Crombie IK. Distribution of malignant melanoma on the body surface. Br J Cancer 1981;43:842-9.
[25]Crombie IK. Variation of melanoma incidence with latitude in North America and Europe. Br J Cancer 1979;40:774-81.
[26]Weinstock MA, Colditz,BA, Willett WC, Stampfer MJ. Bronstein, BR, Speizer FE. Nonfamilial cutaneous melanoma incidence in women associated with sun exposure before 20 years of age. Pediatrics 1989;84:199-204.
[27]Tucker MA, Goldstein AM. Melanoma etiology: where are we? Oncogene 2003;22:3042-52.
[28]Berwick M, Armstrong BK, Ben-Porat L, Fine J, Kricker A, Eberle C. Sun exposure and mortality from melanoma. J Nat Cancer Inst 2005;97:95-199.
[29]Veierød MB, Weiderpass E, Thörn M, Hansson J, Lund E, Armstrong B. A prospective study of pigmentation, sun exposure, and risk of cutaneous malignant melanoma in women. J Natl Cancer Inst 2003;95:1530-8.
[30]Oliveria S, Saraiya M, Geller A, Heneghan M, Jorgensen C. Sun exposure and risk of melanoma. Arch Dis Child 2006;91:131-8.
[31]Elwood JM, Gallagher RP, Hill GB, Pearson JCG. Cutaneous melanoma in relation to intermittent and constant sun exposure—the western Canada melanoma study. Int J Cancer 2006;35:427-33
[32] Grant WB. Role of solar UV irradiance and smoking in cancer as inferred from cancer incidence rates by occupation in Nordic countries. Dermatoendocrinol. 2012;4(2):203-11.
[33]Setlow RB, Woodhead AD, Grist E. Animal model for ultraviolet radiation induced melanoma: platyfish-swordtail hybrid. Proc Natl Acad Sci 1989;86:8922-9026
[34]Adams S, Lin J, Brown D, Shriver CD, Zhu K.Ultraviolet Radiation Exposure and the Incidence of Oral, Pharyngeal and Cervical Cancer and Melanoma: An Analysis of the SEER Data. Anticancer Res. 2016 Jan;36(1):233-7.
[35]Garland FC, White MR, Garland CF, Shaw E, Gorham ED. Occupational sun exposure and melanoma in the USA Navy. Arch Environ Health 1990; 45:261-67.
[36] Rivers, J. Is there more than one road to melanoma? Lancet 2004;363:728-30.
[37] Crombie, I. Racial differences in melanoma incidence. Br J Cancer 1979;40:185-93.
[38] Elwood JM, Gallagher RP, Hill GB, Pearson JCG. Cutaneous melanoma in relation to intermittent and constant sun exposure – The Western Canada melanoma study. Br J Cancer 1985;35:427–33.
[39]Maldonado JL, Fridlyand J, Patel H, Jain AN, Busam K, Kageshita T, Ono T, Albertson DG, Pinkel D, Bastian BC. Determinants of BRAF mutations in primary melanomas. J Natl Cancer Inst 2003 Dec 17;95(24):1878-90.
[40]Shuster, S. Is sun exposure a major cause of melanoma? No. BMJ2008;337:a764
[41]Garsaud P, Boisseau-Garsaud AM, Ossondo M, Azaloux H, Escanmant P, Le Mab G. Epidemiology of cutaneous melanoma in the French West Indies (Martinique). Am J Epidemiol 1998;147:66-8
[42]Godar DE, Landry RJ, Lucas AD. Increased UVA exposures and decreased cutaneous Vitamin D3 levels may be responsible for the increasing incidence of melanoma. Med hypothesis (2009), doi:10.1016/j.mehy.2008.09.056
[43]Grant, W. An ecologic study of cancer mortality rates in Spain with respect to indices of solar UVB irradiance and smoking. Int J Cancer 2007;120:1123-28.
[44] Tuohimaa P, Pukkala E, Scélo G, Olsen JH, Brewster DH, Hemminki K, Tracey E, Weiderpass E, Kliewer EV, Pompe-Kirn V, McBride ML, Martos C, Chia KS, Tonita JM, Jonasson JG, Boffetta P, Brennan P. Does solar exposure as indicated by the non-melanoma skin cancers protect from solid cancers? Vitamin D as a possible explanation. Eur J Cancer 2007;43:1701-12.
[45]Grant, W. Solar ultraviolet irradiance and cancer incidence and mortality. Chapter 2. Edited by JorgReichrath, Landes Bioscience 2007.
[46]Grant, W. Solar ultraviolet irradiance and cancer incidence and mortality. Chapter 2. Edited by JorgReichrath, Landes Bioscience 2007.
[47] Kline & Company’s Cosmetics & Toiletries USA Annual Service (1972 and 2008 editions).
[48] Fredonia market research group report, 2009.
[49] Matsuoka LY, Ide L, Wortsman J, MacLaughlin JA, Holick MF. Sunscreens suppress cutaneous vitamin D3 synthesis. Journal of Clinical Endocrinology & Metabolism 1987; 64:1165-68.
[50] Garland CF, Garland FC, Gorham ED. Could sunscreens increase melanoma risk? Am J Public Health 1992;82(4):614-5.
[51] Garland CF, Garland FC, Gorham ED. Rising trends in melanoma. An hypothesis concerning sunscreen effectiveness. Ann Epidemiol 1993 Jan;3(1):103-10.
[52] Shuster, S. Is sun exposure a major cause of melanoma? No. BMJ2008;337:a764
[53] N.J. Levell, C.C. Beattie, S. Shuster and D.C. Greenberg. Melanoma epidemic: a midsummer night’s dream? British J Dermatol 2009;161:630–34
[54] Ackerman, B. The Sun and the “Epidemic” of Melanoma: Myth on Myth. 2008.
[55]ArgenzianoG1, Cerroni L, Zalaudek I, Staibano S, Hofmann-Wellenhof R, et al. Accuracy in melanoma detection: a 10-year multicenter survey.J Am Acad Dermatol. 2012 Jul;67(1):54-9.
By Marc Sorenson,, EdD. Sunlight Institute…
The medical properties are terrific! A new study from the University of Kansas demonstrates that children born to women who receive more sun exposure during the second trimester of pregnancy, have a considerably lowered risk of asthma later in life.[1] The researchers did not look at sunny geographical areas vs. areas of little sun to make their assessments, but rather looked at different amounts of sunlight occurring in the same areas in different years. They found that in areas that had experienced high quantities of sun in a given year, the risk of asthmatic children being born in that year was reduced, that is, if their mothers experienced that sun exposure during the second trimester of pregnancy.
The researchers theorized that higher levels of vitamin D during sunny times accounted for the protective effects of sunlight. That may be true, but the protection may have occurred from sun exposure per se, independent of vitamin D. One of the most recent studies on factors that contribute to asthma showed that living in a room without windows was associated with an increased the risk of asthma of 930%, and living in an area without adequate sun was associated with an increased the risk of 220%.[2] Considering that windows filter out the UVB light that stimulates the production of vitamin D, having windows could not have reduced asthma by vitamin D production—it had to be some other factor—something that entered the room through that window glass–protected the people with windows from the remarkable increase in asthma they would have otherwise had. We know that UVA light, which does pass through windows, stimulates the production of nitric oxide, which is a potent vasodilator. Could it also be a bronchodilator? This explanation, of course, is theory.
Whatever the reason, the study on sunlight and pregnancy is just one of many that have indicated a protective effect of sun exposure against asthma. Safely embrace the sun, and tell pregnant mothers to do the same. It could enhance the quality of life for their children later on, and reduce the cost of health care for all of us.
[1] http://www.biospace.com/News/asthma-free-it-might-be-because-of-moms-sunny/413945
[2] Kamran A, Hanif S, Murtaza G. Risk factors of childhood asthma in children attending Lyari General Hospital. J Pak Med Assoc 2015 Jun;65(6):647-50.
By Marc Sorenson, EdD Sunlight Institute
Those of us that understand the importance on regular sun exposure on human health were not surprised by the most recent research by Dr. Pelle Lindqvist and colleagues. It showed that women who had active sun-exposure habits lived longer than those who did not.[1] Over a 20-year period, the study demonstrated that compared to the highest sun-exposure group, life expectancy of sun avoiders was reduced significantly. Much of the reduction in death among the sun-exposed group was due to a lessened risk of cardiovascular disease and non-cancer, non-cardiovascular death. The risk of skin cancer was slightly increased among the sun exposed group, primarily because they lived longer and had more time to contract cancer.
Perhaps the most impressive statement to come out of the research was this: “Nonsmokers who avoided sun exposure had a life expectancy similar to smokers in the highest sun exposure group, indicating that avoidance of sun exposure is a risk factor for death of a similar magnitude as smoking.”
This newest research is just one of several important contributions by Lindqvist and his group. Other assessments of the 20-year study revealed that the subjects who avoided sun exposure were twice as likely to die of any cause compared to those who had the highest sun exposure, and the researchers made this statement: “In both models the summary sun exposure variables showed a ‘dose-dependent’ inverse relation between sun exposure and all-cause death.”[2]
The research also showed that women with “normal” sun exposure habits were not at significantly increased risk of either melanoma or melanoma-related death. The publication seemed to give vitamin D most of the credit for increased life spans among those who had high sun exposures, but also mentioned the possibility that nitric-oxide production by sun-exposed skin may have been a factor.
If avoiding the sun is as dangerous as smoking cigarettes, why do many dermatologists still try to frighten us to death about soaking up some rays? Will they never learn?
[1] Lindqvist PG, Epstein E, Nielsen K, Landin-Olsson M, Ingvar C, Olsson H. Avoidance of sun exposure as a risk factor for major causes of death: a competing risk analysis of the Melanoma in Southern Sweden cohort. J Intern Med. 2016 Mar 16. doi: 10.1111/joim.12496. [Epub ahead of print].
[2] Pelle G. Lindqvist, Elisabeth Epstein, Mona Landin-Olsson, Christian Ingvar, Kari Nielsen, Magnus Stenbeck & Håkan Olsson. Avoidance of sun exposure is a risk factor for all-cause mortality: results from the Melanoma in Southern Sweden cohort. J Intern Med. 2014 Jul;276(1):77-86.
By Marc Sorenson, EdD Sunlight Institute…
Leukemia is a cancer of the bone marrow that prevents the normal manufacture of red blood cells, white blood cells and platelets. It can lead to infection, impaired blood clotting and anemia. The good news is that embracing the sun may have a profoundly protective effect against this deadly disease.
Consider this research by Dr. Timo Tomonen and his colleagues that showed a very close relationship between sun deprivation and acute myeloid leukemia.[1] The researchers stated that “During the light season, the incidence decreased by 58% (95% confidence interval, 16–79%) per 1,000 kJ/m2/d increase of solar radiation.” In Finland, It has also been shown that deficiency of sunlight (and perhaps cold weather) was associated with excessive diagnoses when compared to diagnoses in in the sunlit, warm season. Other research has indicated that sun exposure during mothers’ pregnancies reduced the risk of leukemia and other cancers in their children.[2]
Finally, in a laboratory study using UVA irradiation of leukemia cells, it was found that such radiation caused rapid apoptosis (natural cell death) in the exposed cells.[3] UVA, of course, is the major ultraviolet component of the solar radiation that reaches the earth. UVA also has been shown to cause a marked decline in the proliferation of leukemia cells.[4] Proliferation is the process of rapid growth and multiplication of cancer cells. So it appears that sun exposure has two more positive attributes for preventing cancers: it has the ability to hasten the death of cancer cells and to retard the tendency of cancer cells to grow and multiply out-of-control. It is also interesting to note, although the researchers did not mention it, that UVA exposure does not cause the production of vitamin D, which means that some other mechanism of sun exposure was responsible for the positive results. Vitamin D is a wonderful photoproduct of sun exposure, but positive benefits of other photoproducts are available. When we substitute vitamin D supplements for sun exposure we may make a critical mistake and increase our risk of leukemia and other diseases. Nothing is a match for habitual, safe sun exposure, but sun lamps would be a close second.
The sun is a natural protector against leukemia. What more need we say?
[1] Timo Timonen, Simo Näyhä, Tapani Koskela, Eero Pukkala. Are sun deprivation and influenza epidemics associated with the onset of acute leukemia? Haematologica 2007; 92 (11):1553-56.
[2] Christina Lombardi, Julia E. Heck, Myles Cockburn, and Beate Ritz. Solar UV Radiation and Cancer in Young Children. Cancer Epidemiol Biomarkers Prev 2013;22:1118-1128.
[3] Zhuang S, Kochevar IE. Ultraviolet A radiation induces rapid apoptosis of human leukemia cells by Fas ligand-independent activation of the Fas death pathways. Photochem Photobiol. 2003 Jul;78(1):61-7.
[4] Leszczynski D, Fagerholm S, Leszczynski K. The effects of the broadband UVA radiation on myeloid leukemia cells: the possible role of protein kinase C in mediation of UVA-induced effects. Photochem Photobiol. 1996 Dec;64(6):936-42.
By Marc Sorenson, EdD. Sunlight Institute
Part of our brain function is influenced by a naturally produced protein called Brain-Derived Neurotropic Factor (BDNF), part of a cascade of proteins that promotes neuron growth and prevents neuron death.[1] Research shows that BDNF has an influence on processes and behaviors such as depression and brain plasticity and has a seasonal variation in concentration that correlates with the amount of ambient sun;[2] BDNF increases in the spring and summer and decreases in fall and winter. The authors of this research summed up their findings thusly: “This finding is important for our understanding of those factors that regulate BDNF expression and may provide novel avenues to understand seasonal dependent changes in behavior and illness such as depression.”
Correct levels of BDNF, however, have many other important and positive effects in the body,[3] including promoting of long-term memory, regulation of mood and perception of pain, reduction of Alzheimer’s disease and Huntington’s disease, and control of epilepsy, depression, anxiety, bipolar disorders, schizophrenia and addiction. In addition, it has positive effects on type-two diabetes, cardiovascular disease and colorectal cancer.
BDNF has been shown to increase significantly after bright light exposure,[4] and in what I would consider to be a remarkably important study, both light exposure and treadmill exercise increased the expression of BDNF in rats,[5] or as the researchers showed, exercise and/or bright light promoted neurogenesis (new nerve cell growth) in the adult rat brain. How important is this finding for adults who are worried about cognitive decline? We are actually seeing an example of new brain cells being built by bright light and exercise. But the researchers were not through with their recommendations. They stated this in their summary: “In view of these findings, we propose that moderate exercise or exposure to sun during childhood can be beneficial for neural development.”
Other research has also indicated that physical activity is positively associated with BDNF.[6]
Add one more natural chemical that is inversely associated with depression and directly associated with sun exposure. We now have vitamin D, serotonin, endorphins, dopamine and BDNF.
Want to maintain your IQ and other brain functions? Would you rather not take the chance of suffering from Alzheimer’s? Embrace the sun, and move your body! Be careful not to burn. And remember that the use of sunscreens may negate many of the sun’s wholesome effects.
[1] http://scicurious.scientopia.org/2010/12/13/bdnf-and-depression/
[2] Molendijk ML, Haffmans JP, Bus BA, Spinhoven P, Penninx BW, Prickaerts J, Oude Voshaar RC, Elzinga BM. Serum BDNF concentrations show strong seasonal variation and correlations with the amount of ambient sun. PLoS One. 2012;7(11):e48046.
[3] Juzeniene A. Beneficial effects of UV‐radiation unrelated to Vitamin D. Presentation at International Symposium Biological Effects of Light June 11 ‐ 12, 2015 Homborg, Germany.
[4] Tirassa P, Iannitelli A, Sornelli F, Cirulli F, Mazza M, Calza A, Alleva E, Branchi I, Aloe L, Bersani G, Pacitti F. Daily serum and salivary BDNF levels correlate with morning-evening personality type in women and are affected by light therapy. Riv Psichiatr. 2012 Nov-Dec;47(6):527-34.
[5] Kwon SJ, Park J, Park SY, Song KS, Jung ST, Jung SB, Park IR, Choi WS, Kwon SO. Low-intensity treadmill exercise and/or bright light promote neurogenesis in adult rat brain. Neural Regen Res. 2013 Apr 5;8(10):922-9.
[6] Gomes da Silva S, Arida RM. Physical activity and brain development. Expert Rev Neurother. 2015 Aug 9:1-11.
By Marc Sorenson, EdD, Sunlight Institute…
A new investigation from Chinese researchers demonstrates that sun exposure is dramatically protective against Parkinson’s disease (PD).[1] The paper reported a study in which 201 newly diagnosed patients were compared with 199 controls who were free of PD. Data on vitamin D intake, blood vitamin D levels and sun exposure were obtained in both groups by using a self-report questionnaire.
For blood vitamin D levels, those who had the highest levels had a 48% lowered risk of PD; for sun exposure, those receiving the greatest exposure had about 47% reduced risk of PD.
Whereas a significant positive correlation existed between blood levels of vitamin D and sun exposure, vitamin D intake from supplements, food, etc. did not correlate to blood levels of vitamin D.
This is a particularly interesting study in that it demonstrates that vitamin D should be raised by exposure to the sun when possible rather than dietary intake. It appears that dietary intake the amounts most people receive is not effective for raising those levels.
The evidence for a protective effect of sun exposure against PD has been building for some time. In 1988, it was observed that when four northern census regions of the U.S. were compared with three southern regions, death rates for PD were significantly higher in the northern regions,[2] indicating a possible protective effect of sun exposure. Later research corroborated those findings, demonstrating a strong north-south decreasing gradient for PD among whites.[3]
There are several more studies indicative of a positive effect of sun on PD, and these will be included in the book on sunlight that Dr. William Grant and I are writing, and which we hope to have published in May. Stay tuned, and safely embrace the sun!
[1] Juan Wang, Deyu Yang, Yu Yu, Gaohai Shao and Qunbo Wang 2. Vitamin D and Sunlight Exposure in Newly-Diagnosed Parkinson’s Disease. Nutrients 2016;8:142.
[2] Kurtzke JF, Goldberg ID. Parkinsonism death rates by race, sex, and geography. Neurology. 1988 Oct;38(10):1558-61.
[3] Lanska DJ. The geographic distribution of Parkinson’s disease mortality in the United States. J Neurol Sci. 1997 Sep 1;150(1):63-70.