
Sepsis and septicemia, major killers that associate with sun deprivation. By Marc Sorenson, EdD

Sepsis facts:
Sepsis is an infection of tissues by bacteria, and septicemia is a form of sepsis that infects the blood. Septicemia is a severe and often deadly blood infection. Noxious bacteria attack tissue or blood, and when they die or when their cell walls rupture, they release poison (endotoxin). So, these dying organisms may do more harm than the bacterial attack itself. In addition, the disease accounts for 500,000 emergency-room hospital visits per year in the USA. And, it is followed by a typical stay of 6 to 9 days.[1] As a result, it is one of the worst medical conditions. And, it often results in multiple organ failure and death. There are about 750,000 cases per year, and about 3% of all hospital admissions result in a case of sepsis. Read more.
Sepsis and hospitals
Hospitals are hotbeds of antibiotic-resistant “superbugs” and other infectious agents. In cases of severe sepsis, antibiotics have not improved survival. In fact, antibiotics may produce molecules that exacerbate sepsis.[2] Therefore, the health system must urgently find and implement non-antibiotic solutions to this crisis.
Also, it should be remembered that sunlight is said to be the best disinfectant.[3] The annual cost of care for sepsis is about $17 billion. And, in the case of severe sepsis, antibiotics have not improved survival. In fact, it is especially relevant that antibiotics may produce molecules that exacerbate it.[4] Sepsis is one of the top-ten causes of death and the second leading cause of hospital-associated deaths. So only coronary intensive care units end up having more deaths. In North America, sepsis and its related disorders kill more hospitalized people than heart attacks, colon cancer, breast cancer or AIDS.
Dr. William B. Grant’s research with sepsis and septicemia.
Dr. William Grant hypothesized that vitamin D deficiency, due to inadequate sun exposure, is a risk factor. That is true for both sepsis and septicemia.[5] He points out that septicemia incidence is also highest in winter and lowest in the autumn. Another point is that rates are highest in the Northeast (low sunlight) and lowest in the Southwest (high sunlight).[6] Therefore, all of this leads to the idea that sun deficiency is a major cause this disorder.

Consequently, sun deficiency could play a strong causal role in the disease, since deficiency inhibits the production of cathelicidins. Cathelicidins are antimicrobial peptides which facilitate the destruction of pathogenic germs’ cell walls, leading to their death. In addition, these peptides also help inactivate the endotoxins released as a result of that destruction.[7], [8], [9]
Stay well and thereby avoid hospitals (and sepsis).
Finally, it would be best to avoid hospitals and their superbugs. The formula? Obtain some regular, non-screened, non-burning sunlight around noon when available. Happy sunning! And be sure to read my new book, Embrace the Sun.
[1] http://www.summitmedicalgroup.com/library/adult_care/ac-sepsis_dx/
[2] Mookherjee N, Rehaume LM, Hancock RE. Cathelicidins and functional analogues as antisepsis molecules. Expert Opinions on Therapeutic Targets 2007;11:993-1004
[3]http://sunlightinstitute.org/tag/sepsis/.
[4] Mookherjee N, Rehaume LM, Hancock RE. Cathelicidins and functional analogues as antisepsis molecules. Expert Opinions on Therapeutic Targets 2007;11:993-1004.
[5] Grant, WB. Solar ultraviolet-B irradiance and vitamin D reduce the risk of septicemia. Dermatoendocrinol 2009;1:37-42.
[6] Danai PA, Sinha S, Moss M, Haber MJ, Martin GS. Seasonal variation in the epidemiology of sepsis. Crit Care Med. 2007;35:410–15.
[7] Giacometti A, Cirioni O, Ghiselli R, Mocchegiani F, D’Amato G, Circo R, Orlando F, Skerlavaj B, Silvestri C, Saba V, Zanetti M, Scalise G. Cathelicidin peptide sheep myeloid antimicrobial peptide-29 prevents endotoxin-induced mortality in rat models of septic shock. Am J Respir Crit Care Med 2004;169:187-94.
[8] Giacometti A, Cirioni O, Ghiselli R, Bergnach C, Orlando F, D’Amato G, Mocchegiani F, Silvestri C, Del Prete MS, Skerlavaj B, Saba V, Zanetti M, Scalise G. The antimicrobial peptide BMAP-28 reduces lethality in mouse models of staphylococcal sepsis. Crit Care Med. 2004;32:2485–90.
[9] Cirioni O, Giacometti A, Ghiselli R, Bergnach C, Orlando F, Silvestri C, Mocchegiani F, Licci A, Skerlavaj B, Rocchi M, Saba V, Zanetti M, Scalise G. LL-37 protects rats against lethal sepsis caused by gram-negative bacteria. Antimicrob Agents Chemother. 2006;50:1672–9
 New book, Embrace the Sun, recommends non-burning sun exposure, citing research on sun exposure, vitamin D, and disease risk.
New book, Embrace the Sun, recommends non-burning sun exposure, citing research on sun exposure, vitamin D, and disease risk.
Available on Amazon, Embrace the Sun, by authors Marc B. Sorenson, Ed.D. and William B. Grant, Ph.D., claim that sun avoidance may be nearly as hazardous to your health as cigarette smoking! Will there soon be a Surgeon General’s warning about staying indoors or putting on too much sunscreen? Is this book based on science or pure science fiction?
The book is based on science and research. Together, Sorenson and Grant have worked 62 years studying and practicing health, nutrition, and the proper relationship with sunlight. A mountain of evidence exists showing that sunlight can promote weight loss, reduce depression, and profoundly decrease the risk of today’s common diseases including most cancers, heart disease, autism, diabetes, osteoporosis, multiple sclerosis, infertility, preterm birth and psoriasis. Do I have your attention? This book provides solid evidence towards a case for regular, sensible sun.
“Marc Sorenson and Bill Grant take us on a delightful journey to better understand the health benefits of our magnificent sun at a time when our sun has been demonized by various health organizations, including the dermatology community, which has been essentially unchallenged for the past 50 years,” said Michael F. Holick, Ph.D., M.D., Boston University Medical Center, “Embrace the Sunis an easy read that is chock-full of valuable information about the health benefits of sensible sun exposure. It provides a very practical guide on how to take advantage of our Magnificent Sun.”
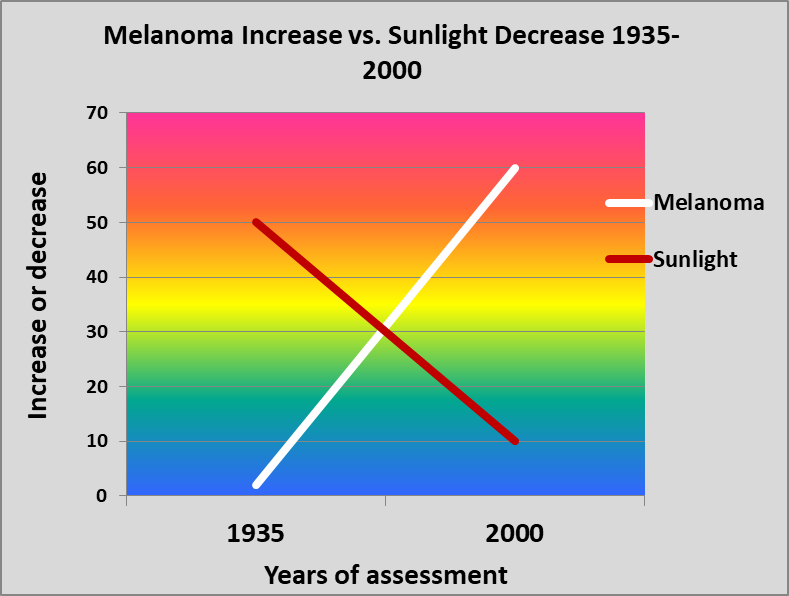 According to the book, 75% of all melanomas occur on areas of the body that are seldom or never exposed to sunlight. Additionally, sun exposure has decreasedby about 90% in the U.S. population since 1935. During that same period, melanoma incidence has increasedexponentially, by approximately 3,000%! This evidence debunks the myth that melanoma is caused primarily by the sun, and instead suggests that the disease is at least partially caused by sun deprivation.
According to the book, 75% of all melanomas occur on areas of the body that are seldom or never exposed to sunlight. Additionally, sun exposure has decreasedby about 90% in the U.S. population since 1935. During that same period, melanoma incidence has increasedexponentially, by approximately 3,000%! This evidence debunks the myth that melanoma is caused primarily by the sun, and instead suggests that the disease is at least partially caused by sun deprivation.
“This book is a tour de force for health effects of exposure to the sun,” said Cedric F. Garland, Dr. Ph. F.A.C.E., University of California at San Diego. “It is written simply enough and in such a light-hearted vein that any intelligent fifth grader can and should read it. It also should be required reading for every upcoming doctor in training and all health care professionals.”
Sorenson and Grant prepare the reader to make an informed choice. With summer coming, is it wise to get out regularly at midday, exercise, and soak up some rays? Or better to stay indoors, continuing the current regimen? Could it be that something so central to nature, the sun, which has been part of the human race for thousands of years is now bad for us? In this blip that is the late 20thand beginning 21stcentury has sun avoidance been helpful or hurtful? Read Embrace the Sun and find out!
About Marc B. Sorenson, Ed. D.
Dr. Sorenson is a doctor of education (EdD) with a health background. He and his wife, Vicki, developed one of the world’s top resorts (National Institute of Fitness). During 20 years, their clients lost over 100 tons of fat; two thirds of diabetic guests were freed of medication in two weeks; and others recovered from cholesterol, arthritis, and myriad additional maladies. Sorenson has written ten books and hundreds of blogs for his site, Sunlight Institute. On the recommendation of Senator Orrin Hatch, a flag was flown over the U.S. Senate building to honor his contributions to world health.
About William B. Grant, Ph.D.
Dr. William Grant is an epidemiologist and founder of the nonprofit organization Sunlight, Nutrition and Health Research Center. Grant holds a PhD in Physics from UC Berkeley and worked as a senior research scientist in the field of optical and atmospheric sciences at SRI International, JPL, and NASA Langley.
He published the first paper linking dietary factors to risk of developing Alzheimer’s disease in 1997. Since 2000, he has focused on ultraviolet-B (UVB) radiation and vitamin D and their relation to cancer and other diseases. He has written over 256 peer-reviewed articles, editorials, and letters to the editor on vitamin D and health.
MS prevention by sunlight. By Marc Sorenson, Ed.D. Sunlight Institute
What is MS?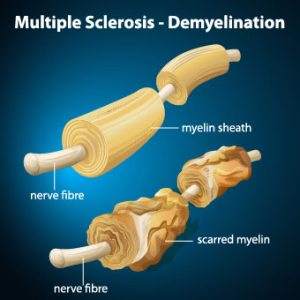
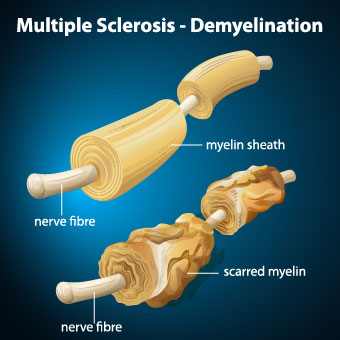
MS is a painful, debilitating, crippling, disease in which immune cells initiate an inflammatory response against myelin. Myelin is the nerves’ protective cover. It is rather like an electric wire that has lost its rubber cover. So, this process, known as demyelination, leaves the nerves bare and susceptible to “short circuiting.” From 85 to 170 people per 100,000 in the USA suffer from MS, and the rate among women, during the period from 1991 through 1994, has increased by 50% compared to the period from 1982 through 1986. Also, as of 2010, the last year for which we could find statistics, there were 350,000-400,000 cases diagnosed in the USA.
There is no doubt that sunshine reduces the risk of MS, because The risk of multiple sclerosis in far northern areas, where there is little sunshine, is more than 100 times greater than it is in equatorial areas. So, in those areas, where sunlight is intense, due to directness of the sun, the rate of MS approaches zero. [1], [2], [3]
And do you know anyone who suffers from multiple sclerosis? They should probably read this blog and then obtain plenty of non-burning sun exposure.
The latest Research on MS, sun exposure and vitamin D.
A study carried out in Southern California corroborates the sun exposure benefits to MS reduction.[4] First of all, the researchers recruited members of three different ethnicities (blacks, Hispanics and whites). In addition, they further divided those ethnicities into those who suffered from MS (known as cases) and those who were free from the disease (controls). They then simultaneously examined lifetime sun exposure and blood vitamin D levels, accounting for genetic ancestry and other factors. The results were impressive:
- Among blacks, the highest lifetime sun exposure was associated with a 47% lower risk, independently of blood levels of vitamin D.
- Among whites, the highest lifetime sun exposure was associated with a 32% lower risk. In this group, highest vitamin D levels also associated with a lower risk of MS.
- Among Hispanics, the highest lifetime sun exposure was associated with a 34% lower risk, independently of blood levels of vitamin D.
This is just the latest research to determine that sun exposure lessened the risk of MS independently of vitamin D. In addition, researchers used animals with experimental autoimmune encephalomyelitis (EAE) (an experimental form of MS). It was induced in animals in a lab setting and then used to determine the relative influences of UVR and vitamin D on MS. In conclusion, they stated, “These results suggest UVR [sun] is likely suppressing disease independent of vitamin D production. Thus, vitamin D supplementation alone may not replace the ability of sun (UV) to reduce MS susceptibility.”[5]
More on sunlight and MS from the same researchers
Later on, some of these same researchers investigated the mechanism by which sun exposure suppressed the disease and determined that UV light selectively inhibits spinal cord inflammation and demyelination.[6]
Furthermore, in another study, scientists performed an investigation with UVR. UVR is the same radiation emitted by the sun and sunbeds or sunlamps. It was administered to animals with EAE.[7] First of all, the researchers found that UVR treatments stopped inflammation and demyelination of the spinal cord. It did so by inhibiting a chemical known as a chemokine, also known as a cytokine. Cytokines are specialized proteins that are either inflammatory or anti-inflammatory in their nature. Therefore, inflammatory cytokines or chemokines are the cause of inflammation and autoimmune attacks resulting in MS. In addition, UVR directly initiated the MS-ameliorating effects, independent of vitamin D.
To conclude:
Finally, as wonderful as vitamin D is, we should realize this: The production of vitamin D is only one of the profoundly healthful effects that are due to Sun Exposure. Hence, those who take vitamin D and believe they will derive all the benefits of sun exposure, are wrong. Consequently, they could be “dead wrong” in the case of a scourge like MS. So, be sure to obtain your full share of non-burning sunlight whenever possible. It could save your life. And, it could save the lives of those who have the disorder or who might be susceptible to it. Maybe we should start paying more attention to our sun exposure?
This is one of many blogs that I and others have written on this subject. In addition, here are a few more that may interest you:
http://sunlightinstitute.org/research-shows-sun-exposure-thwarts-multiple-sclerosis-ms/
http://sunlightinstitute.org/a-vitally-important-study-on-sunlight-and-multiple-sclerosis-ms/
Embrace the sun! Without burning, of course
[1] Alter M, Yamoor M, Harshe M. Multiple sclerosis and nutrition. Arch Neurol l974;31:267-72.
[2] Kurtkze, J. Geography in multiple sclerosis. J Neurol 1977;215:1-26.
[3] Hayes CE, Cantorna MT, DeLuca HF.Vitamin D and multiple sclerosis. Proc Soc Exp Biol Med 1997;216:21-27
[4] Langer-Gould A, Lucas R, Xiang AH, Chen LH, Wu J, Gonzalez E, Haraszti S, Smith JB, Quach H, Barcellos LF. Nutrients. 2018 Feb 27;10(3).
[5] Becklund BR, Severson KS, Vang SV, DeLuca HF. UV radiation suppresses experimental autoimmune encephalomyelitis independent of vitamin D production. Proc Natl Acad Sci U S A. 2010;107:6418-23.
[6] Wang Y, Marling SJ, Beaver EF, Severson KS, Deluca HF. UV light selectively inhibits spinal cord inflammation and demyelination in experimental autoimmune encephalomyelitis. Arch Biochem Biophys. 2015 1;567:75-82
[7] Wang Y, Marling SJ, Beaver EF, Severson KS, Deluca HF. UV light selectively inhibits spinal cord inflammation and demyelination in experimental autoimmune encephalomyelitis. Arch Biochem Biophys. 2015 1;567:75-82.

Two recent scientific analyses show that years of negative press about sunbeds has been misleading at best and mendacious at worst.
By Marc Sorenson, Ed.D.
After years of being told there is “no such thing as a safe tan”, new research is showing that exposure to sunbeds, those that mimic sunlight, may have been healthful all along. Many problems have existed with the research used to frighten the people away from sunlight and sunbeds. Two recent peer reviewed papers have exposed the lack of scientific accuracy by large organizations—organizations that appear to have pursued not the truth, but an agenda bent on discrediting the use of sunbeds. These disclosures were published in Anticancer Research, the Journal of the International Institute of Anticancer Research. The writers concluded that two reports, one by the World Health Organization (WHO) and a second European report called the SCHEER were unbalanced, biased and inaccurate. It is exceptionally important to understand that neither of these reports were peer reviewed. To me, this indicates that they were opinion pieces, not science. The authors of the first paper in the International Journal of Cancer Research and Treatment concluded their findings regarding the WHO and SCHEER thusly: “The stance taken by both agencies is not sufficiently supported by the data and in particular, current scientific knowledge does not support the conclusion sunbed use increases melanoma risk.” The authors of the second paper in the same Journal came to a similar conclusion after doing their analysis of the reports: “Current scientific knowledge is mainly based on observational studies with poor quality data, which report associations but do not prove causality. At present, there is no convincing evidence that moderate/responsible solarium [sunbed] use increases melanoma risk.” It’s almost as if the WHO and Scheer reports, with their twisted reasoning, were making a ridiculous argument, analogous to the following: Water causes drowning; swimming takes place in water; therefore, swimming causes drowning. None of this, of course, is meant to imply that humans should expose themselves to enough water to drown. Neither should they tan excessively. Tanning, like all other activities should be done in moderation, in other words, in a non-burning fashion.
Governments rely on research to advise the public regarding products and services. If there is a perceived risk, then they move forward with legislation to protect the consumer. But suppose that the researchers from WHO and SCHEER have already made up their minds on the risks and benefits of a product? The next step is to prove what they think they already know. That is not science! They accept every piece of research that might lend credence to their hypothesis, and they disregard or denigrate any research that disproves their hypothesis. They make sure that any benefits are removed or discredited. Of course, this allows them to form a conclusion that matches their hypothesis. This has happened with both sunlight and sunbeds. The concern about the risk of skin cancer has stopped agenda-driven “scientists” from even considering the remarkable benefits attributable to sunlight. This has given the world a biased and wholly unbalanced message.
An international group of 16 researchers headed by Professor Dr. Jörg Reichrath, Deputy Director of the Department of Dermatology, Venereology and Allergology at Saarland University Hospital in Homburg/Saar came together to review these reports that they believed to be unbalanced, biased, and full of confounders and inaccuracies. They also believe that the reports have downplayed the benefits of sunbed exposure.
Since most people don’t have the time to read the complete research paper, here are some interesting findings from the papers that I’d like to share with you. These are direct quotes from each paper:
Reichrath et al 2018
- In conclusion, both the SCHEER (1) and WHO (2) reports claim to assess health effects of sunbed use. Unfortunately, however, as such they are partially unbalanced and inaccurate. Both documents mainly assess negative health effects of UV exposure, conceal the large body of evidence demonstrating beneficial health effects of UV radiation, and major conclusions drawn are not sufficiently supported by current scientific knowledge. It should be emphasized that the main conclusions drawn by the SCHEER (1) and WHO (2) reports are not in accordance with generally accepted principles of evidence-based medicine, they not only are not in line with recommendations of the Oxford Centre for Evidence-based Medicine
- …the resulting evidence levels and grades of recommendation are not “strong”, as inaccurately stated in the SCHEER report (which used a highly questionable classification of evidence levels) (1), but are very weak (e.g. level 3a− for systematic reviews of case–control studies with heterogeneity, and grade of recommendation D for outcome “ever” vs. “never” use of a solarium). In conclusion, our present scientific knowledge does not support the notion that sunbed use per se may increase melanoma risk.
- It further underlines the unbalanced view of the SCHEER and WHO reports, that they conceal the large body of evidence demonstrating beneficial health effects of UV radiation.” And “The SCHEER and WHO reports do not adequately consider the large body of evidence demonstrating the negative health consequences of vitamin D deficiency.
- The most known and well-documented beneficial health effects of UV radiation are mediated via vitamin D. However, other factors might be involved, indicating that preventing and treating vitamin D deficiency may not account for all beneficial effects of solar or artificial UV exposure.”
- “Therefore, we rebut these conclusions by addressing the incomplete analysis of the adverse health effects of UV and sunbed exposure (what is‘safe’?) and the censored representation of beneficial effects, not only but especially from vitamin D production.
- While these reports were purportedly based on the best available scientific evidence, we are deeply concerned about their scientific quality and obvious lack of objectivity, most likely owing to an infusion with the laudable zeal to combat alarming increases in skin cancer. Both publications show an implicit tendency toward an unbalanced view and must be criticized because of many scientific misinterpretations and shortcomings.
- Several meta-analyses of poor quality consolidate the observational study data and compound the flaws of these studies.
- For example, dermatological phototherapy is often included when only sunbed use should be assessed [e.g. Landi et al.], and in many studies, subgroups of individuals with presumably high UV exposure in the past (e.g. individuals with history of ‘non-melanoma skin cancer’ or ‘dermatological conditions’) are excluded from controls but not cases (control selection bias).
- Additionally, it should be noted that studies available are characterized by high heterogeneity and by difficulties in adjusting for important confounding factors, including solar UV and lifestyle: only a minority of studies report odds ratios (ORs) adjusted for the same confounding factors, 12 studies not for a single confounder.
- Moreover, because individual confounders were assessed using different interrogations, these studies are only partly comparable limiting the ability to interpret results of a combined estimate. And these results should not be considered reliable (56).
- In this context, the same results and risk estimates as given in Boniol et al. (44) and
- Colantonio et al. could well be obtained in the following scenario, as indicated elsewhere. Sunbed use has no effect on melanoma risk, lifestyle factors such as extensive sunbathing in the summer as a sun worshipper or an ‘unhealthy lifestyle’ (e.g. alcohol, smoking use), do increase melanoma risk with true OR=1.2 (it has been reported previously that sun worshippers and individuals with an ‘unhealthy lifestyle’ go more frequently to tanning salons
- Many of the confounding factors, including extensive sunbathing in the summer and unhealthy lifestyle, have not been adequately and systematically considered in studies performed to date. For example, the comparison of sunbed users to non-users is confounded by their lifestyle habits, with typical sunbed users found to be females who tend to smoke cigarettes and drink alcohol more frequently than non-users, as well as eating less healthy food.
- Both the SCHEER and WHO reports underappreciate the large body of evidence from epidemiological and animal studies that demonstrates no increase in melanoma risk following chronic (moderate) UV exposure.
- Many other studies also support the concept that sub-erythemal exposure to UV doses not only does not increase melanoma risk, but may even be protective.
- It further underlines the unbalanced view of the SCHEER and WHO reports, that they conceal the large body of evidence demonstrating beneficial health effects of UV radiation.
- Moreover, epidemiological evidence provides support for solar UVB protection against a number of cancer types, including breast, colorectal, lung, ovarian, pancreatic and prostate cancer.
- Moreover, reductions of melanoma mortality rates during the past decades do not support the hypothesis that UV radiation from sunbeds may have increased melanoma risk.
- It has been suggested that better detection methods have been in use to detect melanoma earlier, which is also a possible reason for the increased risk that has been observed.
- Unfortunately, however, as such they are partially unbalanced and inaccurate. Both documents mainly assess negative health effects of UV exposure, conceal the large body of evidence demonstrating beneficial health effects of UV radiation, and major conclusions drawn are not sufficiently supported by current scientific knowledge.
- With this unscientific approach, both the SCHEER (1) and WHO (2) reports are not adequate and do not properly summarize current knowledge on comparing beneficial and adverse effects of UV exposure from sunbeds.
Burgard et al 2018
- “Moreover, in our opinion, the attempts of Boniol et al and others to attribute melanoma cases to solarium use are speculative and scientifically not sufficiently supported.”
- “As many as 35.5% (n=11) of all the included studies did not account for a single confounder.”
- Overall, quality of included studies was poor as a result of severe limitations, including possible recall and selection bias, and due to lack of interventional trials.
- However, for all outcomes analyzed, overall study quality and resulting levels of evidence (3a−) and grades of recommendation (D) were low due to lack of interventional studies and severe limitations including unobserved or unrecorded confounding.
- Many studies have investigated the impact of indoor tanning on melanoma risk (8-59), however, most of them have been criticized for limitations, unbalanced view, errors or incorrectness (11, 17). While some reports suggest that solarium use may increase melanoma risk (e.g. 19, 29, 32), other investigations found no or even a protective effect (e.g. 20-22, 24, 35).
- It should be emphasized that the results of these cohort and case–control studies represent associations and do not prove causality.
- According to the Oxford Centre for Evidence based Medicine, for the outcome ever-exposure to UV radiation from a solarium, we determined an evidence level of 3a− (systematic review of poor quality cohort and case–control studies) and a grade D of recommendation.
- As an example, incorrectness in one of the main findings of the study of Boniol et al. (8) forced the authors to publish a correction (16). As Colantonio et al. point out, comparison of five previously published systematic reviews on this topic demonstrates an alarming tendency for copying data without referencing the original article, and without checking for errors (11).
- As an example, the influential review of the IARC Working group published in 2007 (10) has been criticized for numerous errors in content and typography [e.g. giving wrong numbers for the controls reported 1989 by MacKie et al. (38) and 1981 from Adam et al. (19)], which are also present in two subsequent reviews (11). Furthermore, the numbers of participants from several included studies (31, 43) published in the IARC review could not be derived by us and others (11) from the original articles.
- Moreover, in our opinion, the attempts of Boniol et al. (8) and others (12) to attribute melanoma cases to solarium use are speculative and scientifically not sufficiently supported.
- For recruitment before 1991, a higher OR [increased risk] was found as compared with recruitment from 1991-1999 or since 2000.
- Moreover, both the resulting level of evidence and grade of recommendation of studies investigating the association of melanoma risk with solarium use are weak.
- In summary, our review has highlighted the poor quality of the evidence available at present on this topic. We conclude that (i) results of our and previously published meta-analyses most likely overestimated the association of melanoma risk with solarium use, (ii) both the level of evidence and grade of recommendation of studies published previously investigating the association of melanoma risk with solarium use are weak, and therefore (iii) present scientific knowledge does not support the hypothesis of an increased melanoma risk due to solarium use, and questions studies that try to attribute melanoma cases to indoor tanning, and does not support initiatives that aim to ban responsible/moderate solarium use for tanning purposes.
Sadly, some “science” follows the paths of deception. Many writers have let a bias toward a particular outcome color their judgement and even misinterpret their results. You can find many examples of bad science by doing an internet search for that term. Because a result was printed in a scientific journal, or stated by a multinational organization, it does not necessarily denote truth.
As you can see, the 2 reports on sunbeds have concluded that sunbeds were dangerous and would lead to cancer. The research compiled to reach this conclusion was of poor quality and biased. It also left out relevant information—information that would have completely changed the result. Obviously, these results were born of a need to produce the result they wanted, not a need to find the truth.
The statement, that there is no need to use sunbeds, as there are no health benefits, is an egregious misstatement of the facts. Here are several citations that belie the idea that there are no health benefits of sunbed use:
- Vitamin D production and bone strength.
In a study comparing 50 subjects who used a sunbed at least once a week to 106 control subjects who did not use sunbeds, it was shown that tanning-bed users had 90% higher 25(OH)D levels than non-users, and that they also had significantly higher bone-mineral density, indicative of stronger bones.[1] Another study showed that whereas a daily 400 IU vitamin D supplement did not maintain healthful 25(OH)D levels, sunbed use increased 25(OH)D levels by 150% in only seven weeks.[2]
- Sunbeds can control psoriasis and eczema.
They are often recommended by dermatologists as a way to overcome these diseases. Scientists have stated that UV light is nearly 100% effective for many dermatologic conditions, and that sunbeds are very convenient sources of UV rays for patients who cannot otherwise afford the rigorous travel and time commitments necessary to visit the dermatologist.[3] This was the conclusion they reached: “Unsupervised sun exposure is a standard recommendation for some patients to obtain phototherapy. Selected use of commercial sunbeds in the treatment of dermatologic conditions may be another useful and effective treatment for those patients with an inability to access office-based or home-based phototherapy.”
- Sunbed use reduces chronic pain.
A study of pain in fibromyalgia patients, conducted by dermatologists, revealed that those who used UV-producing sunbeds experienced a decrease of 0.44 points on a 10 point scale (Likert scale) determined by subject questionnaire, when compared to those who did not receive UV light.[4], [5]
- Sunbeds may reduce endometrial cancer. Research from Sweden demonstrated that women who use sunbeds more than three times yearly had a 40-50% reduction of the risk for endometrial cancer.[6] The authors surmised that the effects observed were likely due to stimulating higher 25(OH)D levels in winter.
- Sunbed use reduces the risk of clots. In an eleven-year study of the sun-exposure habits of 40,000 women, venous thrombotic (clotting) events were measured. It was found that women who sunbathed during the summer, on winter vacations, or when abroad, or used a sunbed, had a 30% decrease in the risk of clots compared to those who did not sunbathe.[7] The authors again speculated that increased vitamin D, which has anticoagulant properties, had provided these positive results.
- Sunbed use is associated with lower breast-cancer risk.[8]
- Perhaps the most important research on sunbeds was a 20-year study in Sweden by Dr. Pelle Lindqvist and his colleagues, who showed that women who used sunbeds were 23% less likely to die from any cause than women who did not use them.[9] This research also showed that low sun exposure as a risk factor for all-cause death was comparable in magnitude to smoking, and women with active sun exposure habits were found to live 1 to 2 years longer as compared to those with the lowest sun exposure habits.
I couldn’t agree more with the latest research.
[1] Tangpricha V, Turner A, Spina C, Decastro S, Chen TC, Holick MF. Tanning is associated with optimal vitamin D status (serum 25-hydroxyvitamin D concentration) and higher bone mineral density. Am J Clin Nutr 2004;80:1645-49.
[2] Holick, M. Boston University. “Effects Of Vitamin D And Skin’s Physiology Examined.” Science Daily 21 February 2008 <http://www.sciencedaily.com¬ /releases/2008/02/080220161707.htm>.
[3] Radack KP, Farhangian ME, Anderson KL, Feldman SR. A review of the use of tanning beds as a dermatological treatment. Dermatol Ther (Heidelb). 2015 Mar;5(1):37-51.
[4] Kaur M, Feldman SR, Liguori A, Fleischer AB Jr. Indoor tanning relieves pain. Photodermatol Photoimmunol Photomed. 2005 Oct;21(5):278.
[5] Taylor SL, Kaur M, LoSicco K, Willard J, Camacho F, O’Rourke KS, Feldman SR. Pilot study of the effect of ultraviolet light on pain and mood in fibromyalgia syndrome. J Altern Complement Med. 2009 Jan;15(1):15-23.
[6] Epstein E, Lindqvist PG, Geppert B, Olsson H. A population-based cohort study on sun habits and endometrial cancer.Br J Cancer. 2009 Aug 4;101(3):537-40.
[7] Lindqvist PG, Epstein E, Olsson H. Does an active sun exposure habit lower the risk of venous thrombotic events? A D-lightful hypothesis. J Thromb Haemost. 2009 Apr;7(4):605-10.
[8] Yang L, Veierød MB, Löf M, Sandin S, Adami HO, Weiderpass E. Prospective study of UV exposure and cancer incidence among Swedish women. J Intern Med. 2014 Jul;276(1):77-86
[9] Lindqvist PG, Epstein E, Landin-Olsson M, Ingvar C, Nielsen K, Stenbeck M, Olsson H. Avoidance of sun exposure is a risk factor for all-cause mortality: results from the Melanoma in Southern Sweden cohort. J Intern Med. 2014 Jul;276(1):77-86.
What is the truth about melanoma? A news report from Seattle laments that in spite of exceptionally cloudy weather, the state of Washington has one or the highest melanoma rates in the nation.[1] Melanoma incidence there increases about 2% per year.

On top of this, they admit that most of the melanoma occurs on the cloudy west side of the state, and that the risk of melanoma has tripled in the last thirty years. Other states with cloudy weather have the same problems. The report further states that one should cover up with sunscreen no matter how cloudy and dark the weather, or even if one is spending the day indoors.
The reason? One of those awful sun rays may find its way through the clouds and then penetrate a window! What’s next? Must I slather myself with sunscreen before crawling in bed at night and then set my alarm for four hours later to wake up and reapply? This sunscreen mania now verges on insanity.
Sunscreens are said to have been invented in 1936 by Eugene Schueller, the founder of L’oreal, and ten years later a suntan cream was invented.[2] In that year, it is unlikely that many people used the sunscreen, but let’s suppose that one bottle was used that first year. Let us further suppose that three billion bottles are now used each year. That is probably a very low estimate.
In 1935, one in every 1,500 people contracted melanoma.[3] Today, one in 50 contract melanoma.[4] In other words, there has been a 30-times (3,000%) increase in the risk of melanoma, accompanied by a spectacular increase in sunscreen use that probably reaches into the billions of percent. Sunscreens have not helped prevent melanoma.
Here is what I would like to say to the people of Seattle: Each year, more and more people are taking extra precautions to limit sun exposure and keep their skin protected when outdoors. Why then, do melanoma rates continue to increase? The answer from dermatologists, when confronted by this contradiction, is to avoid the sun even more and to slather our skins with sunscreen 24 hours a day. If we follow that advice, next year melanoma rates will increase even more. Did you realize that this melanoma increase is happening in a time where most of the population is working indoors? Does it intrigue you to learn that each year, as we use more sunscreen and avoid the sun, the risk of melanoma increases?
The latest research also shows that sunscreens are leading to widespread vitamin D deficiency.[5] Among children, vitamin D deficiency is now at alarming levels, having increased 8,300% since 2000 as they are “protected” from the sun’s rays.[6] The reason? Sunscreen can reduce the production of vitamin D by the skin up to 99%.[7]
The research also shows us that sun deprivation leads to 336,000 deaths per year in the U.S.[8] Sun is vital to human health, and too much “protection” can kill us. Here are some facts that you should know about sun exposure and health:
- A 20-year Swedish study shows that sun avoidance is as bad for the health as cigarette smoking.[9] [10]
- A Spanish study shows that women who seek the sun have one-eleventh the hip-fracture risk as those who avoid sun.[11]
- Men who work outdoors have half the risk of melanoma as those who work indoors.[12]
- Women who avoid the sun have 10-times the risk of breast cancer as those who embrace the sun.[13]
- Women who sunbathe regularly have half the risk of death during a 20-year period, compared to those who stay indoors.[14]
- Sun exposure increases nitric oxide production, which leads to a decrease in heart disease risk.[15]
- Vitamin D, the sunshine vitamin, is essential to human survival, and sun exposure is the only natural way to obtain it. Sunbathing can produce up to 20,000 units of vitamin D in 20 minutes of whole-body exposure.[16]
- Sun exposure dramatically improves mood through the production of serotonin and endorphin.[17] [18]
- Sun exposure increases the production of BDNF, which is vital to human health.[19]
The person who wrote the Seattle article is a dermatologist who also says that during his years in Seattle, melanoma risk has tripled.
There are no rational thought processes leading to the advice to use sunscreen all day long, 24/7, in cloudy Seattle. In fact, as pointed out in the research above, exactly the opposite is true.
[1] http://search.aol.com/aol/search?q=paypal%20account&s_it=keyword_rollover&ie=UTF-8&VR=3430
[2] http://www.whenwasitinvented.org/when-was-sunscreen-invented/
[3] Melanoma International Foundation, 2007 Facts about melanoma. Sources: National Cancer Institute 2007 SEER Database, American Cancer Society’s 2007 Facts and Figures, the Skin Cancer Foundation, the American Academy of Dermatology.
[4] American Cancer Society. Melanoma Skin Cancer Overview 9/16/2014. Accessed on 9/23/2014 at http://www.cancer.org/cancer/skincancer-melanoma/overviewguide/melanoma-skin-cancer-overview-key-statistics
[5] Pfotenhauer KM, Shubrook JH. Vitamin D deficiency, its role in heath and disease, and current supplementation recommendations. J Am Osteopath Assoc. 2017; 117(5):301.
[6] Basatemur E, Horsfall L, Marston L, Rait G, Sutcliffe A. Trends in the Diagnosis of Vitamin D Deficiency. Pediatrics. 2017 Mar;139(3).
[7] Matsuoka LY, Ide L, Wortsman J, MacLaughlin JA, Holick MF. Sunscreens suppress cutaneous vitamin D3 synthesis. Journal of Clinical Endocrinology & Metabolism 1987; 64:1165-68.
[8] Baggerly CA, Cuomo RE, French CB, Garland CF, Gorham ED, Grant WB, Heaney RP, Holick MF, Hollis BW, McDonnell SL, Pittaway M, Seaton P, Wagner CL, Wunsch A.L. McDonnell MPH, Mary Pittaway MA, RD, Paul Seaton MS, Carol L. Wagner MD & Alexander Wunsch MD. Sunlight and Vitamin D: Necessary for Public Health. J Am Coll Nutr. 2015;34(4):359-65.
[9] Lindqvist PG, Epstein E, Nielsen K, Landin-Olsson M, Ingvar C, Olsson H. Avoidance of sun exposure as a risk factor for major causes of death: a competing risk analysis of the Melanoma in Southern Sweden cohort. J Intern Med. 2016 Mar 16.
[10] Lindqvist PG, Epstein E, Nielsen K, Landin-Olsson M, Ingvar C, Olsson H. Avoidance of sun exposure as a risk factor for major causes of death: a competing risk analysis of the Melanoma in Southern Sweden cohort. J Intern Med. 2016 Oct;280(4):375-87.
[11] Larrosa M, Casado E, Gómez A, Moreno M, Berlanga E, Ramón J, Gratacós J. Vitamin D deficiency and related factors in patients with osteoporotic hip fracture. Med Clin (BARC) 2008;130:6-9.
[12] Stephen J Merrill, Samira Ashrafi, Madhan Subramanian & Dianne E Godar. Exponentially increasing incidences of cutaneous malignant melanoma in Europe correlate with low personal annual UV doses and suggests 2 major risk Factors. Dermato-endocrinology 2015;7:1.
[13] Bidgoli SA, Azarshab H. Role of vitamin D deficiency and lack of sun exposure in the incidence of premenopausal breast cancer: a case control study in Sabzevar, Iran. Asian Pac J Cancer Prev. 2014;15(8):3391-6.
[14] Pelle G. Lindqvist, Elisabeth Epstein, Mona Landin-Olsson, Christian Ingvar, Kari Nielsen, Magnus Stenbeck & Håkan Olsson. Avoidance of sun exposure is a risk factor for all-cause mortality: results from the Melanoma in Southern Sweden cohort. J Intern Med. 2014 Jul;276(1):77-86.
[15] Weller R. The health benefits of UV radiation exposure through vitamin D production or non-vitamin D
Pathways. Blood pressure and cardiovascular disease. Photochem. Photobiol. Sci. 2016.
[16] Hollis B. Circulating 25-hydroxyvitamin D levels indicative of vitamin D sufficiency: implications for establishing a new effective dietary intake recommendation for vitamin D. J Nutr. 2005;135:317-22.
[17] Lambert GW, Reid C, Kaye DM, Jennings GL, Esler MD. Effect of sun and season on serotonin turnover in the brain. Lancet. 2002 Dec 7;360(9348):1840-2.
[18] Jussila A, Huotari-Orava R, Ylianttila L, Partonen T, Snellman E. Narrow-band ultraviolet B radiation induces the expression of β-endorphin in human skin in vivo. J Photochem Photobiol B. 2016 Jan 7;155:104-108
[19] Tirassa P1, Iannitelli A, Sornelli F, Cirulli F, Mazza M, Calza A, Alleva E, Branchi I, Aloe L, Bersani G, Pacitti F. Daily serum and salivary BDNF levels correlate with morning-evening personality type in women and are affected by light therapy. Riv Psichiatr. 2012 Nov-Dec;47(6):527-34.